Gastroesophageal Reflux Disease (GERD)
The University of Chicago Medicine is home to one of the few centers in the United States that is dedicated to diagnosing and treating esophageal disorders, including gastrointestinal reflux disease (GERD) in adults and children. Our program allows our physicians to specialize in esophageal conditions and help patients with GERD on a daily basis.
Request an appointment for GERD
Providing the very best treatment options for patients is a key priority. We offer a full range of medical, surgical and minimally invasive treatment options to meet each patient’s needs, including minimally invasive GERD surgery that can provide lasting relief without the side effects of taking medications for decades. We continually evaluate the results of our treatment approaches and work to improve surgical and medical solutions for patients.
What is GERD?
Gastrointestinal reflux disease (GERD) is more than just heartburn. Untreated, GERD can develop into more serious conditions, including cancer for a small percentage of individuals.
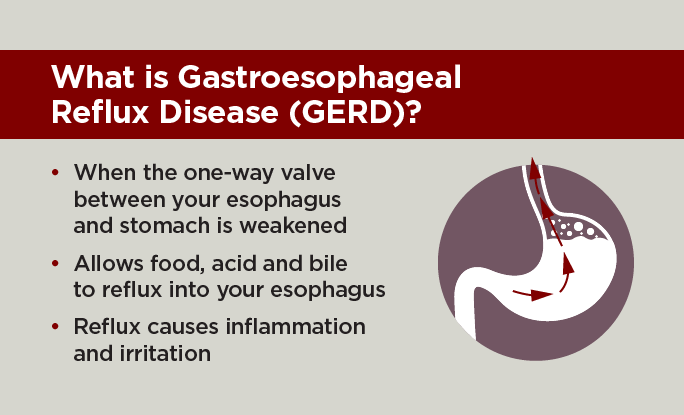
It’s normal to experience gastroesophageal reflux (also known as acid reflux) once in a while after eating. For most people, this acid reflux is a mild form of heartburn that can be controlled with over-the-counter medications, changes in food choices or changes in the quantity eaten at one time. If mild heartburn persists, your primary care doctor may prescribe a stronger medication. In comparison, gastroesophageal reflux disease (GERD) is less common but more troublesome than periodic acid reflux.
Anti-Reflux Treatment Options for GERD
Anti-reflux surgery is very effective for treating gastroesophageal reflux disease. The different anti-reflux operations described below are performed by specialized esophageal surgeons at UChicago Medicine through small incisions using minimally invasive techniques. These procedures all work by recreating the damaged valve between the esophagus and stomach.
Minimally Invasive GERD Surgery
Our expert surgeons at UChicago Medicine with specialized training in minimally invasive techniques use high definition laparoscopy and advanced robotic technology, making anti-reflux surgery a very safe and effective treatment option. These operations are performed using small, less than ½ inch cuts in the skin. This allows for not only less scaring, but also faster and easier recovery and less pain for patients. Using these minimally invasive techniques most patients go home later that day or the next day.
Which GERD surgery is best for me?
Our surgeons understand that every patient is unique. Depending on each your personal goals after surgery, your comfort with the procedure and your overall health, our team will help you make the right choice for you.
The different types of GERD surgeries include:
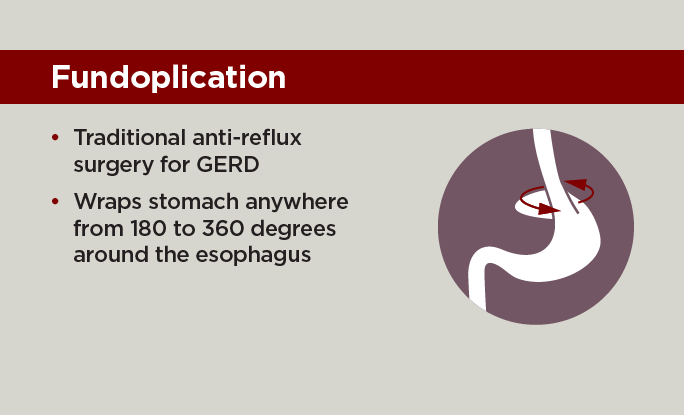
Fundoplication. Fundoplication has been the standard operation for GERD treatment for nearly 50 years. This operation involves a wrap of the stomach around the esophagus to reconstruct the lower esophageal sphincter to function as a one-way valve again.
This wrap of the stomach is called a fundoplication. A fundoplication can be a full 360-degree wrap or a partial wrap ranging from 180 to 270 degree, which allows for the best reconstruction of the valve to control reflux.
The degree of wrapping varies based on the patient and their valve function. We use special techniques to customize this wrap to the patient to prevent the valve from being too tight, but still controlling reflux symptoms.
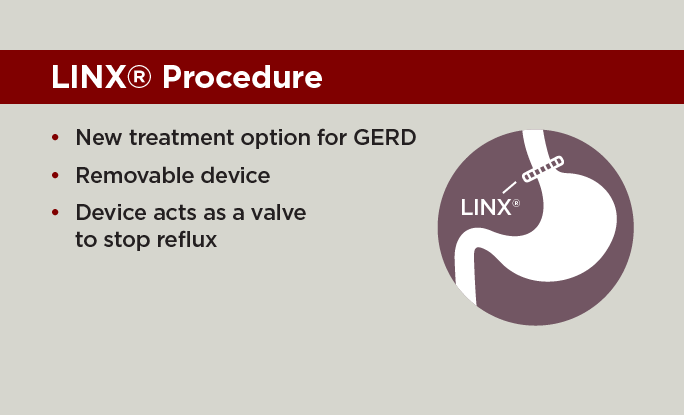
LINX Procedure. The LINX System is a new treatment option for patients with GERD. This removable device is a small, flexible ring of magnetic, titanium covered beads that acts as a valve to stop reflux from the stomach. The LINX system is designed to stay closed at rest to prevent acid reflux back into the esophagus, but then will expand with a normal swallowing mechanism to allow food and drink to pass into the stomach.
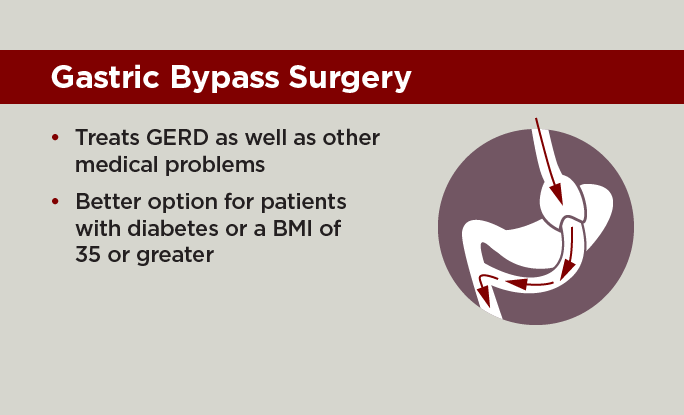
Gastric bypass surgery. Gastric bypass surgery may be an option in a select group of patients that have other medical conditions in addition to reflux. This operation works to treat reflux as well as diabetes, hypertension, sleep apnea, arthritis and allows for dramatic weight loss. Patients with a BMI 35 or higher may be a candidate for this treatment and can be discussed as a treatment option for you.
Transoral Incisionless Fundoplication (TIF). One of the latest options for GERD is called transoral incisionless fundoplication (TIF). This outpatient procedure may be used instead of traditional fundoplication in some patients.
During a TIF, a gastroenterologist inserts a long, thin tube called an endoscope with specially designed instruments down your esophagus to repair your valve without any incisions. Patients who have TIF often have a shorter recovery, compared with traditional fundoplication.

Nationally Ranked in Gastroenterology and GI Surgery
According to U.S. News & World Report's 2023-24 Rankings.
Learn more about U.S. News Best HospitalsTreating five medical problems with one surgery
Gastric bypass surgery was an option for Michael Meadows who had other medical conditions in addition to reflux. This operation works to treat reflux as well as chronic conditions, including diabetes, hypertension, sleep apnea, arthritis and allows for dramatic weight loss.

Request an Appointment
You can also make an appointment with our providers by:
– Scheduling a virtual video visit to see a provider from the comfort of your home
– Requesting an online second opinion from our specialists
To speak to someone directly, please call 1-888-824-0200. If you have symptoms of an urgent nature, please call your doctor or go to the emergency room immediately.
* Indicates required field